
My current interest includes precision medicine, dynamic treatment regimes, machine learning, high-dimensional inference, semiparametric models, survival analysis, electronic health records and clinical trials. I am also interested in developing powerful statistical methods/tools to solve emerging problems for data integration (clinical trials, EHRs, cohort studies) and causal inference (statistical and machine learning methods) that arise from many diseases including infectious diseases, cancer, obesity, cardiovascular diseases, and psychiatric disorders.
Please describe one or two of your most interesting projects.
Project 1: Major depressive disorder (MDD) is a leading cause of disability-adjusted life years and is associated with abnormal reward processing. It remains unclear whether these abnormalities arise from reduced reward sensitivity or impaired learning. Drawing on data from the EMBARC study’s probabilistic reward task, this project proposes a semiparametric inverse reinforcement learning (RL) approach to analyze MDD patients’ reward-based decision-making. The model updates decisions via reward prediction errors weighted by individual learning rates, and models reward sensitivity as a nonlinear, nondecreasing function using I-spline estimation and joint likelihood maximization. Applying to EMBARC, we find similar learning rates but distinct, nonlinear reward sensitivity functions between MDD and control groups. These functions correlate with brain activity in negative affect circuitry during an emotional conflict task.
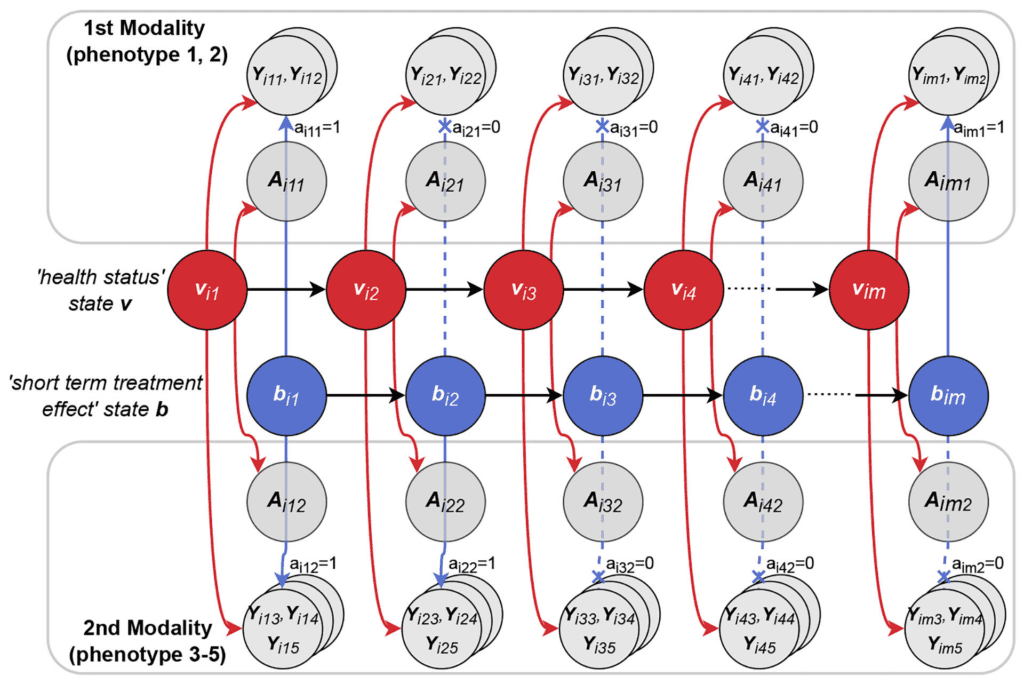
Project 2: Digital technologies can provide frequent, objective, real-world digital phenotypes, but modeling these data is challenging due to confounding and variability from environmental factors and measurement noise. For example, signals on patients’ underlying health status and treatment effects are mixed with variation due to the living environment and measurement noises. Motivated by a Parkinson’s disease mobile health study, this project proposes a mixed-response state-space (MRSS) model to jointly analyze multidimensional digital phenotypes through latent state time series, capturing dynamic health status and treatment effects. The method uses Kalman filtering for Gaussian data and importance sampling with Laplace approximation for non-Gaussian data. The PD mobile health application show MRSS’s effectiveness in remote, real-time digital phenotype analysis.
How did you end up where you are today? (Your research journey)
I obtained my PhD of Statistics from the University of Michigan in 2001, and joined the Department of Biostatistics as a faculty at the University of North Carolina at Chapel Hill. I returned to the University of Michigan as a faculty in the Department of Biostatistics in 2023.
What is the most significant scientific contribution you would like to make?
1. My work develops novel, rigorous methods, algorithms, and theory for semiparametric and nonparametric inference in complex data settings. I have advanced nonparametric maximum likelihood estimation for transformation regression models to analyze univariate and multivariate survival data, as well as joint models for longitudinal and survival outcomes, settings with missing covariates, and problems involving biased sampling. More recently, I have created efficient methods and computationally reliable algorithms that address long-standing challenges in analyzing interval-censored data—including univariate and multivariate interval-censored data and panel count data—and developed efficient semiparametric inference for problems arising in genetic epidemiology, infectious diseases, and mental health and psychiatry.
2. My work develops principled and efficient approaches that integrate traditional statistical inference with modern machine learning to meet emerging challenges in biomedical data science. My 2012 JASA paper introduced machine learning tools such as support vector machines to estimate optimal treatment rules for precision medicine. More recent work addresses challenges driven by high dimensionality, nonlinearity, higher-order interactions, and large-scale data, compounded by missingness, confounding, measurement error, biased sampling, and censoring. A key contribution of my research is the development of statistical and machine learning methods that are theoretically grounded, achieve statistical and computational optimality, and generalize to related settings. For example, in recent work using electronic health records, I developed statistical joint models to characterize disease trajectories and biomarker dynamics, then leveraged these low-dimensional, reproducible mechanistic structures within flexible machine learning frameworks to learn optimal treatment regimens.
3. My work is application-driven, developing methods to solve challenging biomedical problems arising in modern clinical trials, observational studies, and specialized data modalities including medical imaging, genetics, and digital phenotypes. I have designed innovations that strengthen classical statistical inference and expand its utility in these domains. Recent collaborations include biopharmaceutical industry projects on network meta-analysis, adverse event detection, biosimilar evaluation, and long-term COVID-19 vaccine effectiveness. Other work focuses on analyzing high-dimensional, intensive digital phenotype data, including studies of patients with post-traumatic stress disorder.
What makes you excited about your data science and AI research?
As AI has become increasingly powerful in data science, I have grown more fascinated by both its complexity and its remarkable effectiveness. Yet, although many AI algorithms are rooted in foundational statistical principles, I am eager to understand the scientific reasons behind their success and to better align these tools with traditional scientific frameworks. Doing so is essential for ensuring the trustworthiness and generalizability of AI, and for translating its strengths into deeper biomedical insight.