Over the past decade, MIDAS has helped turn AI from a buzzword into a practical tool in medicine,from models that track sepsis risk in the emergency department to a national center that uses AI to design and test drugs more efficiently.
In a busy emergency department, monitors stream a familiar rhythm of numbers: heart rate, blood pressure, oxygen saturation. On a nearby tablet, another signal catches a resident physician’s eye, a rising curve that suggests a patient with vague abdominal pain and a low-grade fever may be heading toward sepsis.
It is not a diagnosis. But it is enough to prompt a closer look, additional tests, or earlier antibiotics if the A clinical picture supports it. In emergency medicine, where minutes matter, that early warning can make the difference between a short hospital stay and weeks in intensive care.

It is not a diagnosis. But it is enough to prompt a closer look, additional tests, or earlier antibiotics if the
A clinical picture supports it. In emergency medicine, where minutes matter, that early warning can make the difference between a short hospital stay and weeks in intensive care.
“The hard part about sepsis is that early on, it can look like a lot of other things,” said Kayvan Najarian, professor of Computational Medicine and Bioinformatics, Emergency Medicine, and Electrical Engineering and Computer Science. “The question is whether we can see deterioration before it becomes obvious.”
Najarian’s lab has spent years developing AI models that do exactly that. Using continuous streams of vital signs and waveforms, the models track how a patient’s risk evolves minute by minute. They rely on tensor based mathematics capable of integrating multiple time series, such as heart rhythms, breathing patterns, and blood pressure fluctuations, into a dynamic picture of clinical risk.
As the models matured, Najarian and his collaborators recognized something important: the same mathematical tools that make sense of noisy, complex physiological data could also be applied far beyond the clinic. The methods developed to track a patient’s shifting trajectory could also be used to untangle biological complexity at other scales: from gene interactions to molecular behavior.
That insight opened a second frontier: drug discovery.
A national hub for data-driven drug development
The Center for Data-Driven Drug Development and Treatment Assessment (DATA), was established in 2021 as a National Science Foundation Industry/University Cooperative Research Center (I/UCRC). DATA is the only I/UCRC focused on using AI to make drug development faster, cheaper, and more reliable; and it complements other drug discovery research on campus and strengthens U-M’s leadership role in this area.
Najarian leads DATA together with H. V. Jagadish, MIDAS Director from 2019 to 2025. The center brings together data scientists, clinicians, pharmaceutical companies, and regulators to work on shared challenges in drug design, toxicity prediction, treatment assessment, and pharmacovigilance.
The stakes are high. Bringing a new drug to market typically takes 10 to 15 years and costs between $1 billion and $2.6 billion. Only about 10 percent of drug candidates that enter clinical trials are ever approved, with most failures occurring late, after enormous investments have already been made.
“The idea is precompetitive research,” Jagadish said. “The research problems are of interest to many pharmaceutical companies, so it makes sense to pool expertise rather than solve them independently behind closed doors.”
Industry partners including Amgen, AbbVie, and Sanofi co-fund research through DATA. Company scientists help select projects and gain access to validated methods, trained talent, and favorable intellectual property terms. DATA fills a national niche for data- and AI-driven drug development, and has already produced new AI technologies for drug discovery and assessment and continues to expand rapidly.
From silos to shared infrastructure
A decade ago, both clinical AI and drug development research looked very different. Clinical AI efforts were often small pilots confined to single hospital units, with limited access to integrated data or validation across sites. Electronic health record data largely sat unused.
“There was a lot of talk about using AI in medicine,” Najarian said, “but very little infrastructure to do it at scale.”
Drug development faced similar fragmentation. Academic labs developed promising algorithms or compounds, but rarely had pathways to test them on industrial datasets. Pharmaceutical companies maintained in-house analytics teams but had little incentive to collaborate on foundational methods.
MIDAS helped change that landscape. “MIDAS gave researchers room to take risks,” Jagadish said. “It helped build a culture where clinicians, engineers, statisticians, and computer scientists could work together.”
Those early investments aligned with broader efforts at Michigan Medicine to operationalize AI responsibly and complemented other central efforts. The AI & Digital Health Innovation group, for example, helped ensure that models developed in research settings could integrate into clinical workflows and align with health system priorities.
On the drug development side, MIDAS played a key role in securing the NSF designation for DATA, positioning the university as a national hub for precompetitive collaboration. DATA developed a Secure Data Hub that allows companies to share encrypted datasets and created federated learning frameworks so models can be trained across multiple databases without data leaving their home institutions.
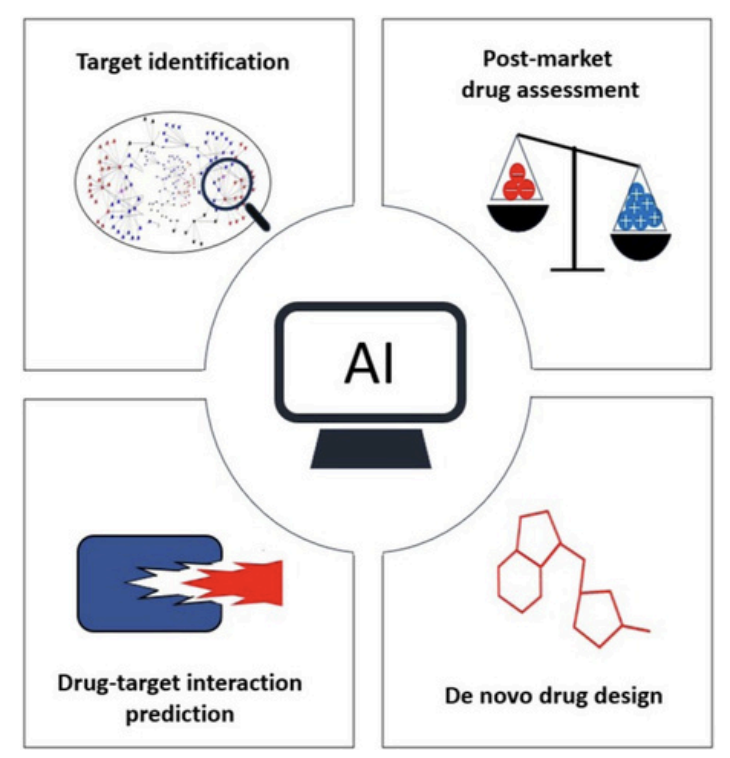
Figure from Minocerri et al. (2025) – AI applications along four critical steps of the DDD process.
Saving time and Saving lives
Back in the emergency department, Najarian’s sepsis trajectory models are designed to act as a “second set of eyes.” They do not replace clinical judgment, but provide continuous risk updates that help clinicians prioritize attention in fast-moving situations. In some cases, earlier identification can mean starting antibiotics an hour sooner, which, in some cases, could make a difference in significantly reducing mortality. AI, when used properly and rigorously, can save lives.
Meanwhile, projects funded by DATA are illustrating how AI can reshape drug development upstream.
One project, led by Duxin Sun in the College of Pharmacy, uses machine learning to analyze preclinical and molecular data and predict safety issues before drugs enter human trials. “If you can predict safety failures early, you save years of work and avoid exposing patients to risky compounds,” Sun said.
Another project, led by Daniel Beard in the Department of Molecular and Integrative Physiology, uses quantitative systems pharmacology models, which means detailed simulations of how drugs affect biological pathways, to predict toxicity arising from emergent system-level effects “We’re moving toward ‘digital twins,’” Beard said, “models that let you test therapies in silico before running human trials.”
Another project, co-led by Peter Tessier in the Department of Pharmaceutical Sciences and Najarian, applies generative AI to design new therapeutic antibodies with improved binding, lower toxicity, and better manufacturability
Privacy, validation, and governance
One of DATA’s most ambitious efforts focuses on privacy-preserving machine learning. In a project led by Najarian, researchers use fully homomorphic encryption, enabling models to train on encrypted data without ever decrypting it. “That unlocks enormous collaborative potential,” Najarian said. “Organizations can work together without exposing sensitive data.”
Pharmaceutical partners gain access to validated methods and talent at lower cost, while regulators and payers benefit from more transparent, rigorously evaluated models for safety and real-world evidence.
Researchers are also acutely aware of equity concerns. Studies at Michigan Medicine, including evaluations of commercial sepsis tools, show that models trained in one setting may perform poorly in others, particularly across different patient populations. “That’s why validation and ongoing monitoring matter, and why DATA regards it as a central focus.” Jagadish said.
Looking ahead
From digital twins to adaptive clinical trials, AI-driven approaches are beginning to shift medicine from describing what is happening to predicting what might happen next. DATA’s national role offers a model for how universities, industry, and government can collaborate on problems too large for any one institution to solve alone.
From emergency department monitors to encrypted drug discovery pipelines, the work reflects a shared belief that AI can make medicine faster and safer, when built, validated, and governed with care.
Another project, led by Daniel Beard in the Department of Molecular and Integrative Physiology,